NAVICULAR STRESS FRACTURES… WHY YOU CAN’T AFFORD TO MISS THEM!!
Navicular stress fractures are one of the most common stress fractures seen in athletes, particularly those involved in explosive activities involving jumping, sprinting, rapid braking/acceleration and changes in direction. The navicular is a crucial bone which is positioned on the medial (inside) aspect of the foot between the forefoot (ball) and rearfoot (heel). It forms the apex of the arch of the foot and, in combination with the surrounding bones, ligaments and tendons, acts to stabilise the foot and assist with efficient foot function.

Signs and Symptoms:
Patients typically present with:
– Poorly localised, midfoot tenderness that is exacerbated by weightbearing in general but in particular certain movements like standing on tip-toes and single leg hopping;
– Pain that can radiate along the medial or dorsal aspect of the foot with the site of maximum tenderness being located commonly in the centre of the proximal dorsal aspect of the bone (known as the N-spot);
– Pain that is alleviated by rest in the early stages; as this condition progresses the pain will remain even after longer periods of rest
Aetiology (Causes):
The mechanism of injury is not conclusive but it has been proposed that the position of the navicular predisposes it to compressive loads from the surrounding bones. Poor ankle joint dorsiflexion and compensatory midfoot pronation typically seen in these individuals have been linked to this condition as they increase the stress on the navicular. If these compressive loads are repetitive and beyond a level that the bone can tolerate then micro-trauma results. Therefore, it is no surprise that this injury is common in sprinters, AFL footballers and fast bowlers.
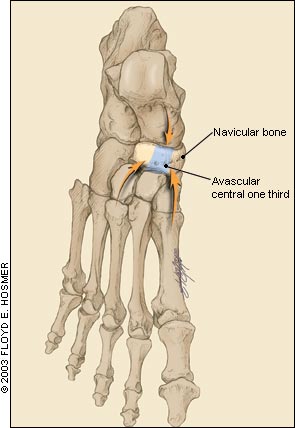
What makes the navicular so susceptible to stress fractures is the poor blood supply to the central part of the bone. A good blood supply is required for bone remodelling therefore, if the bone is under increased load due to high intensity training and/or poor biomechanics, then the ability of the navicular to withstand those loads is reduced. These inherent characteristics of the navicular mean it is classed as a ‘high-risk’ injury due to the potential for delayed healing, non-union of fractures and prolonged time out of sport.
Diagnosis:
Typically, due to the vague nature of patient symptoms, imaging is required to confirm the diagnosis of a stress fracture. MRI is the gold standard due to it’s ability to detect bone oedema and bone stress reaction which are precursors to a stress fracture. CT are also commonly used to grade the severity of the fracture and guide the management of the condition. It is important to note that if the patient displays the clinical signs outlined above then a stress fracture is assumed until proven otherwise.
Treatment:
The treatment of this condition varies based on the severity of the damage. In most cases a period of non-weightbearing immobilisation for 6-8 weeks is enough to allow healing of the bone. The patient will then start a graduated return to activity focused on eliminating any strength imbalances, improving biomechanical function and controlling external factors (training surfaces, dietary inadequacies etc). In cases where delayed healing or displacement of the bone has occurred then surgical intervention may be required. This increases the recovery time with return to sport occurring between 4-5 months after the surgery.
Navicular stress fractures can be a debilitating condition if not managed quickly and appropriately. So, if you are experiencing any pain in the arch or top of your foot see a podiatrist ASAP so an accurate diagnosis and management plan can be implemented to ensure you don’t suffer for too long. To book with one of our podiatrists call our clinic on 94805522 or book online at www.northernpodiatry.com.au
by Mark Whiteside
8